After 44 years in the field of ophthalmic imaging, I recently retired from fulltime practice as a clinical photographer. It was truly humbling when the Penn State Department of Ophthalmology honored my career by publishing a collection of images curated by David Quillen, MD Chair of the Department of Ophthalmology. Here are Dr. Quillen’s words and a link to the collection:
April 1, 2022 marked a significant milestone in the history of Penn State Eye Center: Timothy J. Bennett, longtime ophthalmic photographer, retired following a remarkable career. Mr. Bennett arrived in Hershey in 1994. During his 28-year association with Penn State, he made significant contributions to our patient care, education, and research missions. Ophthalmic imaging is critical in the day-to-day life of an eye practice. Ophthalmic testing—including fundus photography, intravenous fluorescein angiography, optical coherence tomography, fundus autofluorescence imaging—play a significant role in our ability to diagnose and treat patients. In addition to patient care, ancillary studies are essential for our academic teaching and research programs. Mr. Bennett is an exceptionally gifted photographer and his images have been used for countless presentations, journal articles, textbooks, and educational resources. It is no exaggeration to suggest that Penn State Eye Center has one of the highest quality digital image collections in academic ophthalmology.
In addition to his many contributions to Penn State Eye Center, Mr. Bennett is a nationally recognized author, lecturer, and educator in the field of ophthalmic photography. He was named a Fellow of the Ophthalmic Photographers Society (OPS). He has served on the OPS Board of Certification, the OPS Board of Directors, and is Past-President of the OPS. In 2013, Mr. Bennett was awarded the prestigious Outstanding Contributions to Ophthalmic Photography Award, the highest honor bestowed by the OPS. This recognition is awarded to select individuals who have promoted or advanced ophthalmic photography and imaging through their craft, writing, or innovations.
As Mr. Bennett concludes his extraordinary career, I want to highlight a small number of his award-winning contributions to ophthalmic photography. I hope you enjoy the attached digital copy of The Bennett Collection. And please join me in congratulating Mr. Bennett on a remarkable career and thanking him for his many contributions to Penn State Eye Center and the profession of ophthalmic photography. We wish him great peace and fulfillment in his retirement.
Warm regards,
David A. Quillen, MD George and Barbara Blankenship Professor Chair, Department of Ophthalmology Director, Penn State Eye Center
In the past month or so we’ve increased our testing volume after limiting patient visits during a government mandated stay-at-home order during the COVID 19 pandemic. As we’ve ramped back up, we’ve changed our procedures to limit the risk of transmitting the virus. We’ve instituted stringent cleaning protocols, and installed breath shields on some instruments. All clinical personnel now wear PPE (masks, goggles, gloves) and all patients are required to wear masks while in the clinic. We’ve adapted to this “new normal” pretty quickly and our testing volume is almost back to pre-pandemic levels.
Another part of our new normal is a novel clinical finding that seems to be related to the COVID 19 pandemic. Prior to the pandemic, I hadn’t observed this finding. As our numbers increased, I started noticing artifacts that I couldn’t immediately identify in IR fundus images using the Spectralis OCT. I’m wondering how many others in the field have noticed the same thing.
Prominent dark shadow in the infrared fundus image on the left made it challenging to get a good quality OCT image.
This patient came in two weeks ago. Here you see what appears to be vitreous hemorrhage or debris causing a dark shadow that obscures the view in the IR image. I really struggled to get good images. The OCT was adequate, but the accompanying IR fundus image was poor. Those of you that use the Spectralis know that any structure or pathology that is out of focus will typically appear dark because of the confocal pinhole that blocks scattered light from reaching the sensor. So it’s not uncommon to have a compromised view like that if there are media opacities such as dense cataracts, corneal opacities or vitreous pathology, so I didn’t think much of it at first.
But then just two patients later I saw a similar artifact. This time it changed in appearance while I was imaging and got progressively worse. I had the patient sit back and re-positioned.
That seemed to improve the view, but within seconds it deteriorated again and got worse. It almost looked as if I were watching a vitreous hemorrhage occur live. I had the patient sit back yet again, waited several seconds, and resumed imaging. The artifact disappeared again!
Finally, I looked around the device at the patient’s face to see if there was anything I was missing. And then I noticed it, the patient had an ill-fitting mask and was fogging the lens with her breath! The position of the mask forced her breath directly onto the lens surface of the Spectralis. Because of the confocal nature of the Spectralis, the pinhole aperture causes the artifact to appear dark rather than just a simple fogging seen with a slit lamp, fundus camera, or any other non-confocal device.
I asked a few of my astute imaging colleagues about this and a few had seen it but were initially stumped as well. Collectively we now believe we are seeing a new artifact related to patients wearing masks. One of my colleagues thought it was more prominent with the SPECTRALIS 102 degree wide angle lens. That may be because of the different working distance from the patient (closer).
Shadowing on a Spectralis fluorescein angiogram with 102 wide angle lens from breath fog. Image courtesy Gary Miller, CRA, OCT-C, FOPS
Looking back I realized that I had struggled with many patients during the peak of the lockdown. We were only seeing urgent/emergent patients at that time and were not routinely dilating patients in the interest of efficiency. So I assumed the darker fundus images were related to working with smaller pupils. It dramatically effects the confocal fundus image, but not always the OCT image because that component of the device is not confocal. The fogging seems to be more common with certain mask types or on days with high humidity.
Now when it occurs, I often just ask the patient to sit back for a few seconds until the fog clears clears and then resume imaging. Or we sometimes tape the top of the mask to the patient’s nose and cheeks to direct their breath down or to the side.
Changing the OCT working distance to the XL setting may reduce the fogging by changing the angle/distance from the patient’s mask.
Another trick is to change the OCT working distance (XL setting) as if you were trying to capture a longer eye. That effectively changes the angle between the patient’s mask and the front element.
My colleague Gary Miller and I have been unsuccessfully trying to come up with a catchy name for this finding. Here are a few of our attempts, but they’re all pretty lame.
Corona Fog Pandemic haze Mask mist COVID condensation Masquerade artifact
If you have a good one, put it in the comments section.
Here are the current recommendations from Heidelberg on cleaning optical surfaces in their devices. These recommendations seem pretty universal and would likely be similar to those from other manufacturers as well.
Update: A number of people have asked for a document to share whith coworkers. I created a quick pdf adaptation that can be found here.
One of the best ways to ensure high quality ophthalmic diagnostic images is to first establish a rapport with the patient. Once you’ve gained their trust you can easily guide them through the sometimes uncomfortable or stressful process of obtaining information that may determine their diagnosis and influence treatment decisions. Chatting them up a little usually helps to ease their nervousness. This friendly interaction often leads to some interesting conversations.
Patients who undergo ophthalmic imaging for the first time are especially amazed by the whole experience. They are fascinated by the technology used and the incredible images we are able to obtain.
But they also want to know a little about the qualifications needed to perform these tests. They may ask questions like, “What is your job called?” Or, “How long have you been doing this?” “Do you need to be a doctor to do this?” But the most common question I get is, “How did you get into this field?” I usually chuckle and then give them my stock answer, “I’m still trying to figure out how that happened!” I go on to explain it’s not something I set out to do as a profession.
Their next comment is usually, “You must have gone to school a long time, or have a special degree, in order to do this.” They are shocked when I tell them that most people in the field were trained on the job and that there aren’t any specific educational or licensure requirements. It seems to put them at ease when I tell them that I hold multiple certifications in ophthalmic imaging. This speaks to the value of achieving and maintaining voluntary certification.
So how does one get started in this field?
There’s no one “right way” to become an ophthalmic imager. In the absence of formal training or degrees in our profession, most of us learn the majority of the required skills on the job. My background was in commercial photography and I gradually learned enough ophthalmology to apply my photographic skills to imaging the eye. There are many others in the field with a background in photography. Others started as medical assistants or technicians and then learned the photographic side of things on the job. The point is that very few of us set out to become an ophthalmic photographer and one day find ourselves working in the field and learning many of the requisite skills on the job.
One of the problems with OJT is that it is often limited to what is being done in that particular practice setting. To get started in the field or obtain more comprehensive training and expand your skills you may want to take a look at some currently available resources such as text books, online tutorials here on eye-pix.com as well as educational resources through these sources:
Ophthalmic imaging plays a vital role in the documentation and diagnosis, of a wide variety of ocular diseases. It is a fascinating profession, yet obtaining the requisite knowledge and skills to perform diagnostic imaging at a high level can be a challenge. Some of the fundamental techniques and technology used to image the eye have remained the same for many years, but there have been several major advances in the profession over the last two decades. Spectral Domain OCT, fundus autofluorescence, multi-modal imaging, scanning laser ophthalmoscopes, OCT angiography and other techniques have altered the imaging landscape and require that even experienced imagers learn new skills.
There is very little formal education available in ophthalmic imaging, with the notable exception of the ophthalmic imaging curriculum offered at the Rochester Institute of Technology. Graduates of the program at RIT represent some of the most prepared and successful professionals in our field. The vast majority of practitioners in our profession however, do not have this educational foundation. Most of us find it necessary to learn some of the required knowledge and skills through other methods, such as seminars, workshops, handbooks, instrument manuals, and online resources. These are all valuable educational tools, but typically don’t provide a complete educational foundation.
We now have a new resource to help us learn and stay up to date. Ophthalmic Imaging: Posterior Segment Imaging, Anterior Eye Photography and Slit Lamp Biomicrography by Professor Christye Sisson, is an important new educational resource for both novice and experienced imagers. It is the first comprehensive textbook in ophthalmic imaging published in over fifteen years. Our profession really needs a resource such as this, and Professor Sisson is uniquely positioned to create such an educational text. After several years as a clinical ophthalmic photographer, she transitioned into a career as an educator in photography and ophthalmic imaging. She currently serves Program Chair of Photographic Sciences at RIT and this text is based on the curriculum she developed for her students there.
Textbooks can be somewhat analogous to teachers. To be effective they need to be organized, accurate, stimulating, and easy to understand. The organization and layout of this book recognizes the varied career paths for entry into the profession. This text covers fundamentals such as ocular anatomy and photo technology for those just getting started in the field, as well as new technologies that are now dominating our profession. It is exciting to know we have a new “teacher” available to learn the basics of ophthalmic imaging, build new skills, or prepare for professional certification.
I can’t wait to get a look at the final product.
Update 7/1/2018: I received my copy of this text a couple months back and have had time to delve into it more deeply. It is everything that I expected it to be and more. It’s been a useful reference when I wanted to quickly look up topics such as ultra wide-field imaging and scanning laser ophthalmoscopy. I’m sure I’ll continue to reach for it whenever I need a reference in ophthalmic imaging.
Our profession enjoys a long and rich history, one that has seen dramatic advancement in technology and techniques that aid in the documentation and diagnosis of eye disease. My personal interest in the history of ophthalmic photography stems from participation in multiple history symposia sponsored by the American Academy of Ophthalmology’s Museum Committee. In 2011, I was quite honored to be invited to co-chair the symposium Imaging and the Eye, but I think I drew the short straw when we were assigning lecture topics. I was given the task of covering the origins of photography and ophthalmic photography – in a ten minute presentation!
It seemed like a daunting task to somehow cover all that history in such a short talk. But when I started to research the topic, a common theme began to emerge when I came across rivalries, controversies, mistakes, and inconsistencies in the historical accounts related to several important discoveries. Rather than try to force every important milestone or event into a timeline format, I decided to concentrate my lecture on a few important controversies and rivalries. This approach worked well for the symposium, but I ended up with far more material than I could hope to cover in several lectures. And I had barely scratched the surface.
The Pencil of Nature is the first collection of photograph works published in book form by Fox Talbot in 1844. The photographs were printed separately and then mounted or “tipped in”. Talbot claimed that his photographic process preceded that of Daguerre’s in 1839. A digitized version of this book is available through Project Gutenberg.
During the research process, I found that reconstructing history is somewhat like completing a puzzle. Professional historians traditionally have had access to original source documents to support their historical research. Thanks to digital technology, many of these obscure resources are now publicly available through advanced search engines and extensive online collections of scanned historical journals and documents. New pieces of the historical puzzle often become apparent when you can access these primary documents. The accounts in this series benefit from the availability of newly digitized documents, many of which were originally published over 100 years ago. The Internet Archives, Project Gutenberg, and Google Books provide access to digitized, publicly accessible books, periodicals, and journals that are now in the public domain by virtue of their age and expiration of copyright.
Advertisements in The Philadelphia Photographer from June, 1886. Jackman and Webster’s landmark article on the first successful fundus photograph is included in this issue of the photographic periodical. It can be accessed and downloaded from the Internet Archives.
Even with access to these amazing resources, there are still some missing pieces of the puzzle. The available literature sometimes contains conflicting information or apparent mistakes between different historical accounts. Some publications have also proven to be difficult to locate, either online or in print. These hard to find references were often published in the decades just prior to routine digital publication (1960’s & 70’s) and may not yet be eligible for inclusion in public domain collections.
Covers from vintage journals accessed through Google Books. The 1894 Transactions of the Ophthalmological Society of the United Kingdom includes a paper on fundus photography by one of the early pioneers, Lucien Howe. The American Journal of Ophthalmology from 1899 includes a description of Thorner’s reflex-free ophthalmoscope. Thorner and others soon adopted the same optical design to build improved fundus cameras.
In piecing this puzzle together, I found that it pays to read all referenced documents that other historians have cited rather than rely on a citation of a “fact” actually being accurate. Mistakes are sometimes made and then blindly repeated or misinterpreted in other accounts. For example, a non-existent reference title was accidentally published in multiple historical reviews. Listed as “Barr E.: Drs. Jackman & Webster, Philadelphia Photographer June 5, 1886”, it combined fragments of two separate references and was most likely an author’s note to search for them both. 1,2
After searching the online archives, I was able to confirm that the combined title doesn’t exist, yet multiple authors include it in their reference list.3,4 The authors may have also been confused because of a typographical error in multiple references. Elmer Barr was listed as author of an 1887 paper in the American Journal of Ophthalmology, as well as another article in the Scientific American Supplement from 1888.1,5 Both of these articles describe the successful capture of a human fundus photo with more recognizable features than previous investigators. The author’s real name was Elmer Starr, but the typographical error was repeated several times causing an early pioneer in fundus photography to fade into obscurity and lose his rightful place in history. Being able to detect these mistakes and correct the historical record of our profession has been fascinating.
Die Photographie des Augenhintergrundes by Friedrich Dimmer is an atlas of fundus photographs, published in 1907. It contains several amazing reflex-free photographs taken with a one-of-a-kind camera of Dimmer’s own design. This book represents a major milestone in ophthalmic photography. It was digitized by The Internet Archives in 2011 with funding from Open Knowledge Commons and Harvard Medical School.
In piecing these puzzles together, what stood out the most were the often bitter rivalries that seemed to overshadow many of the most important discoveries. Photography was born in the Victorian Era, a time of great discovery, invention, and advancement in science and medicine. The Victorian Era roughly coincided with the Belle Epoch in Continental Europe and the Gilded Age in the United States. It was during this period that Darwin, Babbage, Pasteur, Maxwell, Morse, Helmholtz, and many others made important advancements in science, medicine, and technology. As you will see in future installments of this series, it was also a time of fierce competition, rivalry, and controversy. The brilliant minds of the day often had egos to match their great intellect. The race to be listed as the “first” to discover a scientific breakthrough could become an obsession. Eponyms were popular, and just about every important new discovery was named for the person that first described it.
A classic example of this competition and controversy occurred in the feud over the discovery of anesthesia in the 1840’s when American dentist Horace Wells and his former apprentice William Morton both claimed to be the first to discover the use of inhaled anesthesia. Wells had successfully used anesthesia on several occasions, but was discredited after a famously failed public demonstration. Humiliated after this one failure, he became deeply depressed, began abusing chloroform, and eventually committed suicide. Morton didn’t fare much better. He remained obsessed with recognition throughout his life. He tried to patent ether under a different name, and eventually died penniless. The American Dental Association honored Wells posthumously in 1864 as the discoverer of modern anesthesia, and the American Medical Association recognized his achievement in 1870. Morton was similarly recognized later in life and again posthumously. Both were instrumental in this major medical advancement, but their egos prevented them from sharing in recognition of their achievement.
The next few episodes in this historical series explore similar relationships, rivalries, feuds, and debate surrounding several important milestones in the evolution of ophthalmic imaging. Fortunately the ending of each of these stories is slightly less morbid than the anesthesia saga:
The Priority Debate looks at the frantic race for recognition as the inventor of photography in 1839.
Stereo Photography examines the nineteenth century development of the stereoscope and competing theories on stereo vision that resulted in a bitter feud between Wheatstone and Brewster.
The First Human Fundus Photograph will explore several controversies and professional rivalries in the early days of fundus photography, including how Elmer Starr lost his place in history, as well as another rivalry that led to accusations of falsifying photographic results.
From there we will continue to explore the evolution of ophthalmic imaging by taking a look back at important individuals and events that shaped our field – and hopefully fill in a few more pieces of the historical puzzle that represents the legacy of our profession.
References:
Barr E. On photographing the interior of the human eyeball. Amer J Ophth 1887; 4:181-183
Jackman WT, Webster JD. On photographing the retina of the living eye. Philadelphia Photographer 1886;23:340-341
Van Cader TC. History of ophthalmic photography. J Ophthalmic Photography 1978; 1:7-9
Wong D. Textbook of Ophthalmic Photography. Inter-Optics Publications, New York, 1982
Barr E. Photography of the human eye. Scientific American Supplement 1888; 650:10388
First time viewers of ophthalmic images frequently make the observation that the photos look like something from outer space. Especially when reviewing the round orange retinal photos with their eye doctor, patients often comment, “That looks like the planet Mars.”
Every time it happens I get a chuckle out of it. As if we all truly know what the planet Mars really looks like! But to most people, images of the inside of an eye are foreign and amazing. And there does seem to be a little science fiction aspect to both the appearance of the eye when viewed at high magnification, as well as the technology used to capture these amazing images. There are however, several space analogies that really seem to ring true. Among eye-care professionals, the eyeball is routinely referred to as the “globe”.
Macular Star in a patient with cat scratch neuroretinitis
Many clinical findings are named by their appearance rather than an underlying cause, and several conditions have names derived from their similarity in appearance to objects in space: asteroid hyalosis, macular star, star folds, starry sky, astrocytoma, stellate pattern, etc.
Asteroid hyalosis is comprised of calcium soaps suspended in the vitreous cavity behind the iris. Despite their appearance, most patients with this condition are asymptomatic.
In fact, there are enough conditions like this, that I’ve been able to compile them into the Ophthalmic Jeopardy category: Celestial Bodies.
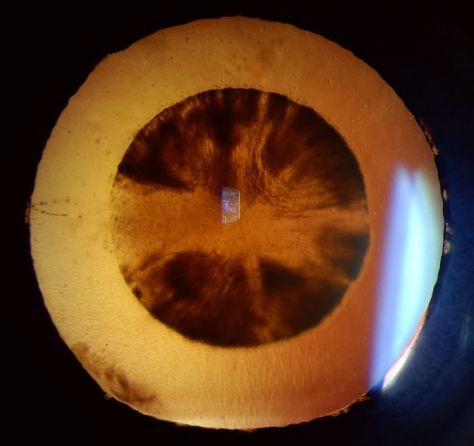
Transillumination of a thinly pigmented iris in a patient with ocular albinism.
Like images from space, there does seem to be an element of wonder and mystery when we peer inside the globe, so in some ways the analogy makes sense.
Cataract
Many ophthalmic images seem reminiscent of photographs from NASA. Or they may stir our imagination or perception of how objects in space might appear.
Lisch nodules on the iris of this patient with neurofibromatosis are reminiscent of peaks, valleys and craters seen in NASA photographs from planets or moons in our solar system.
There are other connections as well. Some of the photographic techniques used by both astronomers and ophthalmic photographers are actually similar. IR capture, interferometry and stereo imaging are common techniques in both fields. The principles of rotational stereo imaging can be applied to both subjects. Filters or lasers of different wavelengths are commonly used to enhance visibility of certain features in both subject types.
Most of these analogies between the eye and outer space, are loose associations rather than a direct connection. There is however, at least one eye condition that can be directly associated with a celestial body. Solar retinopathy is a type of photic injury to the retina that is the result of staring at the sun. This condition typically occurs in patients with psychiatric disorders or under the influence of hallucinogenic drugs.
A case of solar retinopathy with a subtle yellow-white foveal lesion with associated early pigmentary changes.
Some scholars believe that early astronomers, especially Gallileo, went blind as the result of solar retinopathy from viewing the sun through a telescope. It’s important to note that this condition can also occur from viewing a solar eclipse without protective eyewear. The upcoming solar eclipse visible in the U.S. on August 21, may cause a spike in cases of solar retinopathy presenting to emergency rooms and eye clinics. The American Academy of Ophthalmology offers some tips for safe viewing of the eclipse.
In recent years, another connection between outer space and vision has been discovered. It turns out that space travel can have some damaging effects on the human eye. Long-term exposure to microgravity can lead to a hyperopic shift in vision from flattening of the globe. This condition is believed to be related to increased intracranial pressure and is sometimes associated with optic disc edema, cotton wool spots and choroidal folds. Optical coherence tomography (OCT) is used to document changes in thickness of the retinal nerve fiber layer of astronauts before, during, and after space flight.
I took this OCT selfie a few years back when we had a scientist from NASA visiting our clinic while exploring the possibility of putting an OCT on the International Space Station. She wanted to see the Heidelberg Spectralis in clinical use. After demonstrating on several patients, the scientist asked me if I thought it were possible for someone to take an OCT image of themselves. I pivoted the monitor, control panel, and footswitch around so I could operate the OCT from the patient chair and then captured some images of my own retina. I was showing off a little and smugly cautioned the NASA doctor that this was a difficult feat that only an experienced ophthalmic imager could perform. After all, I’ve been doing this for over thirty years. She paused for a moment and then said, “With all due respect, astronauts are some of the smartest and most talented people on earth. They shouldn’t have any difficulty performing OCTs on themselves after a some brief training.” Suddenly I didn’t feel so smug.
A year or so later, the Spectralis arrived at the International Space Station and it looks like she was right. I heard from some colleagues at Heidelberg that the astronauts were given less than 30 minutes of training on the instrument and mastered it quickly!
It’s pretty cool knowing that astronauts are performing ophthalmic imaging on the International Space Station. I wonder if they ever see any resemblance between the eye and celestial bodies?
Disclosure: I have no financial or proprietary interest in the Heidelberg Spectralis.
Here are some links on the condition that’s effecting the vision of astronauts and the use of diagnostic imaging on the space station:
Monochromatic photography has a long history of use in ophthalmology. Illumination of the subject eye with light of a specific color can enhance the contrast and visibility of various structures or findings. Traditionally, it is used in black-and white fundus photography to enhance anatomical details of the retina and choroid, but the same concept can also be applied to other parts of the eye.
Classic example of monochromatic green (red-free) rendition of fundus pathology. The green filter enhances the view to the retinal vessels and the macular lesion.
Monochromatic information can be captured by either filtering the light source (such as with a fundus camera), or placing a contrast filter in front of the camera lens to limit the color reaching the sensor. A subject color will appear lighter when photographed through a filter of the same color, and darker when photographed through a filter of its’ complementary or opposite color. For example, a red subject would appear lighter if exposed through a red filter and darker when photographed a complementary color filter, which in this case would be cyan (blue-green).
Red/Green/Blue color separations of a color fundus photograph of a choroidal nevus demonstrating the value on monochromatic rendering. The red channel shows a darkened lesion similar to the monochromatic effect using a red contrast filter. The blue and green channels suppress the view of the pigmented lesion.
In addition to the traditional technique of using monochromatic illumination with black-and-white photography, another alternative is to take full-color photos without filters and then use software to split the full color image into separate red, green, and blue color components.
Monochromatic views of a salmon colored conjunctival lesion. The lesion appears lighter than the conjunctiva in the red channel, while the blues channel darkens the lesion making it more apparent.
A similar effect occurs in this image of subconjunctival hemorrhage. It’s a great example of how subject colors that are the same as the channel or filter will appear lighter. The blood is darkened by the green and blue channel.
This is a remarkably simple way to obtain monochromatic renderings from any full color image. It works particularly well with color slit-lamp photos of the anterior segment.
A conjunctival lesion stained with lissamine green. Here the red channel darkens the stain pattern, while the green and blue channel lightens the blue-green dye.
One disadvantage to this method is the loss of resolution that occurs when viewing just a single channel that makes up the full color image. It also limits the available monochromatic information to just the three primary colors, red, green, and blue, but that’s usually sufficient for anterior segment applications.
Monochromatic renditions of corneal blood staining.
A dislocated cataract in the anterior chamber. Blue (which is the opposite color of yellow) darkens the lens almost completely, while the red channel enhances its appearance.
The act of learning through a medium that both educates and entertains.
Any of various media, such as computer software, that educate and entertain.
When I am invited to speak at educational meetings, one of the most requested and popular presentation topics is a program titled, Ophthalmic Jeopardy! Based on the popular television quiz show format that most everyone is familiar with, I’ve created an interactive learning experience that also manages to entertain. In short, it’s “Edutainment”. It’s not a new or novel idea, but I’ve taken it a step or two further than similar game show presentations in ophthalmic education. The evolution of Ophthalmic Jeopardy! is interesting.
Years ago, one of the faculty members at the Penn State Department of Ophthalmology approached me about improving our local technician education program. The program included a simple quiz-show format of questions-and-answers with the host reading questions out loud from hand-written cards. It worked, but he wanted to “jazz things up a little”. He told me he had done some online research and found a source for Jeopardy style lockout buzzers/lights that would allow contestants to buzz in when they knew the correct answer. He wanted to pick contestants from the audience and turn it into a competition. Now all he needed was a way to project the questions onscreen and asked if we could make it more interactive like Jeopardy, with onscreen columns of different question-and-answer categories.
I gave it some thought and told him it was possible, but entirely too much work to warrant the effort. But he knew me too well! I gave it a little more thought and started tinkering with the use of hyperlinks in PowerPoint to build an interactive screen that would allow us to randomly move back and forth between categories and questions. I had attended an OPS course entitled “Whiz-Bang PowerPoint Presentations” where Bill Anderson shared a way to hyperlink menus to organize an educational program with easy navigation between multiple speaker presentations. I figured I could build a Jeopardy template using similar hyperlinks between slides.
I converted our existing quiz questions into the Jeopardy answer and question format, but many of them were simple or dry examples. Taking inspiration from Jeopardy! and the sometimes tongue-in-cheek themes, I began accumulating new questions and categories that would entertain as well as test knowledge. In crafting questions, I’ve relied on many years of training and experience in writing questions for certification examinations. But instead of being restricted by the necessary rules for crafting certification questions, Jeopardy allowed me to have some fun and take liberties with some of the topics and content.
Suddenly the project grew and seemed to take on a life of its own. Each presentation contains over 250 hyperlinks, tons of photos, videos, and sound files. We can now chose from an ever growing bank of questions that numbers in the several hundreds! The content is never the same twice. Each time I present it, there are new content areas and questions, but I keep some of the core categories. Often the content will be customized to the specific audience; for example including a local trivia category at regional or international meetings. It’s a great way to review content from other presentations over the course of a day-long or multi day meeting.
In the early days, we would pick contestants who would use the buzzers to buzz in when they knew the answers, we kept score, and gave prizes to the winners. Different faculty members from Penn State Ophthalmology acted as the host and relished playing the part of Alex Trebek. I was the “puppet master” behind the scenes, driving the program and selecting the appropriate hyperlinks to navigate through the questions.
Something was still missing however. It was an entertaining spectacle, but the majority of the audience was reduced to bystanders when we could only chose five contestants from the group. So we eventually opened it up to the entire audience rather than a handful of contestants. At times it can become a little chaotic this way, but everyone seems engaged and involved.
Although we’ve used it at Penn State for audiences ranging from physicians, technicians and the general public, the version used at photography meetings has a higher level of both difficulty and “cheesiness”. Imagers seem to quickly recognize rare and unusual eye findings, but also have a warped sense of humor and “get” the tongue-in-cheek nature of the categories and questions. It works best with larger audiences so it’s become a staple at OPS Mid-Year Educational Programswhere the entire group is together in one lecture hall.
For the last several years, I’ve come out from “behind the curtain” and started hosting Ophthalmic Jeopardy myself. When I retire from ophthalmic photography, maybe I can be a substitute for Alex Trebek! It’s entertaining for sure, but at its core it’s also educational. It’s a fun way to both laugh and learn – in short it’s “Edutainment”!
The concept of edutainment isn’t limited to Ophthalmic Jeopardy. It seems to make it’s way into many of my presentations such as: Stereopalooza, OCT- Anatomy of a Scan, Cases That Tell a Story, Top Ten Uses of a 2×4 in Ophthalmology and others.
For information on how you can be in the audience for the next episode of Ophthalmic Jeopardy!click here.
I’m still feeling a little jet lagged after traveling halfway around the world, but what an amazing trip! Along with over seventy other ophthalmic imagers, technicians, and physicians, I was in Singapore to attend the 2017 International Conference on Ophthalmic Photography (ICOP).
ICOP is a joint educational venture between several ophthalmic imaging organizations including the Ophthalmic Photographers’ Society (OPS) from the United States, the Ophthalmic Imaging Association (OIA) from the UK,the Australian Institute of Medical and Biological Illustrations (AIMBI) from Australia, and the Ooghelkundige Fotografie Nederland (OFN) from the Netherlands. Delegates from 15 different countries were in attendance at this conference.
The three day program was held at the Singapore National Eye Centre (SNEC). The educational program put together by Paula Morris, CRA, FOPS and Sarah Armstrong, CRA, OCT-C, FOPS, included invited lectures, special keynote lectures, and Scientific Paper sessions from dlegates in attendance. Keynote lecturers included Wong Tien Yin, MD, PhD discussing: How a Fundus Photograph Can Save Your Life, Giovanni Staurenghi, MD who presented: Old and New Angiography, Suber Huang, MD who showed amazing images in his lecture: The ASRS Image Bank – a Worldwide Legacy and Gavin Tan Discussing: OCT Angiography – Changing the Way We See.
Photo by Chris Barry, FOPS
I was honored to attend ICOP as not only a delegate, but as an invited lecturer. I ended up presenting all three days of the conference and it was a great honor for me to contribute to the program in this way. I chose topics that I felt would appeal to an international audience and I think it worked out okay. I presented a version of Ophthalmic Jeopardy! that I customized for an audience that was unfamiliar with the namesake television quiz show, that while famous in the U.S., isn’t broadcast in Singapore. Talk about performing a high wire act without a net! I made sure I had some content that everyone could relate to including local Singapore trivia and a review of content covered by presenters in many of the earlier lectures.
The imaging staff at SNEC is renowned for the quality of their ophthalmic photography and they were clearly happy to be hosting this event on their home turf. On a tour of the facility, award winning images were displayed prominently on the walls of the imaging department. It was inspiring to see such an amazing collection of work of the highest quality. Photographers Joseph Ho, Kasi Sandhanam and the rest of the SNEC staff are amazing imagers that are able to balance the efficiency needed to handle a high volume of patients with the highest standards in image quality. They are true professionals in our field.
John Leo with his award winning image. Photo by Chris Barry, FOPS.
Speaking of high quality imaging, the conference also included a photo competition and exhibit that showed some incredible clinical and artistic imaging. Award winners included Sarah Armstrong, Lisa Brealey, Angela Chappell and John Leo.
Photo by Chris Barry, FOPS.
In addition to the educational content during the conference, there were exhibits by a number of sponsoring vendors, some incredible refreshments during the breaks, and a fun evening of food, music, and comradery at the welcome reception.
A highlight of the reception was the photo booth that not only produced mementos of the occasion, but acted as the perfect icebreaker, as spontaneous groups of old friends and new acquaintances would pose together in the spirit of ICOP!
Of course as professional imagers, most attendees had cameras with them and spontaneous selfies were popping up everywhere!
This is the second time that ICOP has been held in this thoroughly modern and spectacular city of Singapore, having previously been hosted here in 1990. And what a great venue for an international conference! Singapore represents an incredible blend of Asian cultures, British influence, modern architecture and great weather.
Like many other delegates I tried to visit as many of the popular sightseeing spots as possible including, Marina Bay, Merlion Park, Super Trees, Sentosa Island, Chinatown, Buddha Tooth Temple, Hawker Markets, the Mt. Faber Cable Car, Henderson Waves, Botanical Gardens and many more. With all these famous sights and numerous museums, there is so much to do and see in this amazing city.
Local residents Paul Chua and Albert Sim took some time to show us some of the local sights in the evenings and recommend the best food stalls in the hawker markets. Joseph Ho hosted an amazing dinner of chili crab at Jumbo Seafood. Alan Wee wrote a great blog post for the OPS/ICOP website with a list and map of places to visit, along with suggestions for some of the best food and coffee shops in the city. It was great having such knowledgeable local guides to help us experience all that Singapore has to offer.
Like many other ICOP delegates, I tried to take in as many of these sights as possible. One of the attractions on my list was the Trick Eye Museum on Sentosa Island which seemed like something an eye imaging professional should check out, at least for a laugh or two. It’s a place where you can take some really cheesy selfies with props and silly scenes in the background! Although I didn’t have time to visit, I walked past and snapped a photo or two. Maybe next time.
ICOP 2017 was an amazing success. Kudos to the international ICOP planning team of Paula Morris, Sarah Armstrong, Chris Barry, Ethan Priel, Becky MacPhee, Angela Chappell and Gerard de Graaf.
The SNEC staff and organizing committee were incredible hosts from Gemmy Cheung, MD, Wong Tien Yin, MD, Gavin Tan, MD, Dr Thiyagarajan Jayabaskar and Lim Hui San, to Joseph Ho, Kasi Sandhanam, and the rest of the imaging and AV teams. They really know how to put on a professional conference.
It was great seeing old friends from around the globe as well as make several new ones.
Photo by Chris Barry, FOPS
Photo by Chris Barry, FOPS
ICOP promotes networking with colleagues and seems to make the world just a little smaller. I believe that each of us found that we all have so much in common no matter how far apart we live. I look forward to the next ICOP which will take place in 2020 at a location yet to be determined.
Along with holidays and festive celebrations, the end of the calendar year often marks the deadline to complete any recertification requirements in order to maintain your professional credentials. I recently completed my OCT-C (Optical Coherence Tomographer-Certified) recertification in December, and just received my updated certificate in the mail. That will hold me for another three years. At the end of 2017, my other professional credential, the Certified Retinal Angiographer, will be up for recertification. It will mark my 30th year of proudly holding the CRA.
I’m not alone when it comes to maintaining these voluntary certifications. Johnny Justice Jr. continues to set an example by maintaining the CRA credential that he originally obtained in 1979 (the first time it was offered). That’s amazing to me. Several others from that inaugural group of CRA recipients, including Peter Hay, Phil Chin, Tom Egnatz, and Chuck Etienne, also maintain their CRA after all these years. None of them have anything to prove at this point in their careers, especially Johnny. He is a pioneer in the profession and was the driving force and founding member of the Ophthalmic Photographers’ Society. He is a well-known author and lecturer, and is universally considered the “Father” of our profession. He certainly doesn’t need the CRA to gain employment, or practice in his chosen profession. He proudly maintains his CRA out of respect for the credential, and what it means to the profession that he helped to create. It clearly has value to him after all these years and all his accomplishments.
In a highly technical field such as ophthalmic imaging it may seem surprising there are no licensure or certification requirements. Certification is strictly voluntary to perform in these roles. It is estimated that less than half the people working as ophthalmic photographers, assistants, or technicians are certified. It’s not easy to obtain certification, and it shouldn’t be. After all it’s meant to identify individuals who have demonstrated a designated level of competence in their field. It takes knowledge, skill, and experience to successfully complete the examination process for certification. Anyone who has completed this process knows the significant effort that is required.
So why get certified if it isn’t required, universally recognized, and takes significant effort? It’s about value. The benefits of certification are often tangible: increased job satisfaction, enhanced job mobility, increased earning power, and a competitive advantage for advancement or the best employment opportunities. But the benefits don’t stop with the certified individual. They also extend to the employer, ophthalmologists, insurers, and most importantly, our patients and their families. All of these groups benefit from knowing they are dealing with a recognized professional.
Certification also helps establish a professional identity and recognition by your peers. It certainly did that for me. In fact, I worked in the field for nearly ten years before initially pursuing certification. I decided it was time to move on in my career and needed certification to gain access to the best jobs. It worked, as my next employer required the CRA as a condition of employment. But I was pleasantly surprised by the additional benefits that certification provided. Although I was very skilled in the technical aspects of photography and had worked at one of the most prestigious institutions in the world, no one outside my place of employment knew my name. That all changed when I obtained my CRA. I suddenly had the respect of my peers and began receiving invitations to play a role in professional activities in the OPS and beyond. Certification seemed to be “the price of admission” to important networking opportunities that lead to leadership roles in the OPS and JCAHPO. From there came many opportunities to share my knowledge through lectures and publication. And it all started with certification.
But the process doesn’t end when you first receive your credentials. Certification is much more than a one-time achievement. It is a dynamic, career-long commitment to continued education, assessment, and professional development. There is incredible value in attaining, and also maintaining, your certification.