This case originally appeared here on eye-pix as a blog post entitled: Mystery Diagnosis: Chairman’s Challenge. It’s a fun read about working through a differential diagnosis as an imager. This is a more succinct version of the same case.
B-scan ultrasonography demonstrated classic highly reflective plaque-like structures with an acoustically empty region behind the tumors.
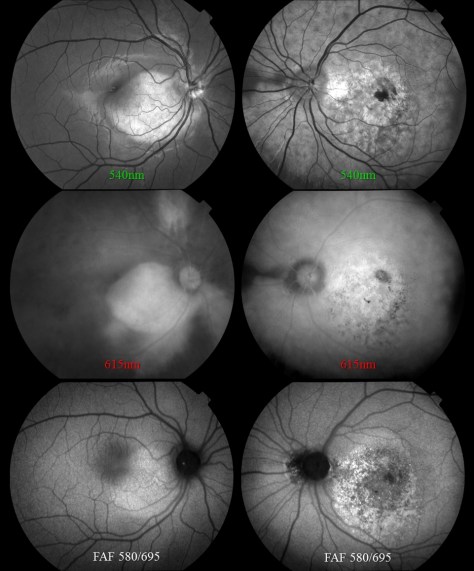
Orange placoid choroidal lesion extending from the optic nerve into the macula. The disc appears hyperemic and there is a small tuft of myelinated nerve fibers on the inferonasal edge.Fundus photograph of the left eye demonstrates a larger, more well defined osteoma with hyperemic disc, macular pigmentary changes, choroidal neovascular membrane and subretinal hemorrhage.OCT of the right eye. The IR fundus image shows a large oval area that is dark from elevation. It’s suggestive of a serous retinal detachment, but the OCT shows no fluid. The retinal pigment epithelium is pushed forward suggesting a choroidal lesion.The OCT of the fellow eye shows significant pigmentary changes, subretinal fluid, and what looks like a choroidal neovascular membrane.Multimodal imaging demonstrates different appearances of the choroidal lesions. Top: monochromatic green shows a stippled appearance of the more advanced lesion in the left eye. Middle: Monochromatic red photos deemphasize the appearance of the retina and retinal vessels. The longer wavelengths penetrate the RPE to emphasize the borders of the choroidal lesions. Bottom: Fundus autofluorescence imaging reveals variable hyperfluorescenc of the lesions probably due to disturbance of the retinal pigment epithelium.B-scan ultrasound shows hyper-reflectivity of the choroidal lesions with posterior shadowing.
Choriodal osteomas are benign ossifying tumors of the choroid composed of mature bone elements. They are relatively rare and are most commonly found in young women. They often demonstrate a thin plaque-like yellow-tan lesion in the macula with sharp, scalloped borders. They are usually unilateral, but can be bilateral. The tumors usually arise adjacent to the optic nerve. Although they have no malignant potential, they may increase in size on serial examination . Symptoms include metamorphopsia, scotoma, and blurred vision. Vision loss may be due to direct tumor involvement or secondary to choroidal neovascularization with subretinal fluid, lipid, or hemorrhage.
Photo-montage comprised of twelve separate fundus images to document the full extent of the lesion in this patient. The standard 45 degree view with the fundus camera wasn’t wide enough to capture the borders of the tumor.
Our patient deferred a fluorescein angiogram to a later date, but was lost to followup. I had previously encountered a similar case nearly twenty years ago. It was before the advent of OCT, but the osteoma was well documented with multi-spectral monochromatic imaging, color fundus photography, fluorescein angiography and B-scan ultrasonography.
A similar case of choriodal osteomal. Color fundus photography shows the classic orange placoid lesion and hyperemic disc. B-scan shows the hyper refelctive nature of the lesion with an acoustically empty behind the tumor. Monochromatic imaging reveals the borders of the lesion. Fluorescein angiography reveals early hyperfluorescence with late staining of the osteoma. There is no evidence of choroidal neovascularization in this patient.
Choriodal osteoma is a rare condition that may present for diagnostic imaging. The appearance is quite striking and can be well documented with several different imaging modalities.