First time viewers of ophthalmic images frequently make the observation that the photos look like something from outer space. Especially when reviewing the round orange retinal photos with their eye doctor, patients often comment, “That looks like the planet Mars.”
Every time it happens I get a chuckle out of it. As if we all truly know what the planet Mars really looks like! But to most people, images of the inside of an eye are foreign and amazing. And there does seem to be a little science fiction aspect to both the appearance of the eye when viewed at high magnification, as well as the technology used to capture these amazing images. There are however, several space analogies that really seem to ring true. Among eye-care professionals, the eyeball is routinely referred to as the “globe”.
Macular Star in a patient with cat scratch neuroretinitis
Many clinical findings are named by their appearance rather than an underlying cause, and several conditions have names derived from their similarity in appearance to objects in space: asteroid hyalosis, macular star, star folds, starry sky, astrocytoma, stellate pattern, etc.
Asteroid hyalosis is comprised of calcium soaps suspended in the vitreous cavity behind the iris. Despite their appearance, most patients with this condition are asymptomatic.
In fact, there are enough conditions like this, that I’ve been able to compile them into the Ophthalmic Jeopardy category: Celestial Bodies.
Transillumination of a thinly pigmented iris in a patient with ocular albinism.
Like images from space, there does seem to be an element of wonder and mystery when we peer inside the globe, so in some ways the analogy makes sense.
Cataract
Many ophthalmic images seem reminiscent of photographs from NASA. Or they may stir our imagination or perception of how objects in space might appear.
Lisch nodules on the iris of this patient with neurofibromatosis are reminiscent of peaks, valleys and craters seen in NASA photographs from planets or moons in our solar system.
There are other connections as well. Some of the photographic techniques used by both astronomers and ophthalmic photographers are actually similar. IR capture, interferometry and stereo imaging are common techniques in both fields. The principles of rotational stereo imaging can be applied to both subjects. Filters or lasers of different wavelengths are commonly used to enhance visibility of certain features in both subject types.
Most of these analogies between the eye and outer space, are loose associations rather than a direct connection. There is however, at least one eye condition that can be directly associated with a celestial body. Solar retinopathy is a type of photic injury to the retina that is the result of staring at the sun. This condition typically occurs in patients with psychiatric disorders or under the influence of hallucinogenic drugs.
A case of solar retinopathy with a subtle yellow-white foveal lesion with associated early pigmentary changes.
Some scholars believe that early astronomers, especially Gallileo, went blind as the result of solar retinopathy from viewing the sun through a telescope. It’s important to note that this condition can also occur from viewing a solar eclipse without protective eyewear. The upcoming solar eclipse visible in the U.S. on August 21, may cause a spike in cases of solar retinopathy presenting to emergency rooms and eye clinics. The American Academy of Ophthalmology offers some tips for safe viewing of the eclipse.
In recent years, another connection between outer space and vision has been discovered. It turns out that space travel can have some damaging effects on the human eye. Long-term exposure to microgravity can lead to a hyperopic shift in vision from flattening of the globe. This condition is believed to be related to increased intracranial pressure and is sometimes associated with optic disc edema, cotton wool spots and choroidal folds. Optical coherence tomography (OCT) is used to document changes in thickness of the retinal nerve fiber layer of astronauts before, during, and after space flight.
I took this OCT selfie a few years back when we had a scientist from NASA visiting our clinic while exploring the possibility of putting an OCT on the International Space Station. She wanted to see the Heidelberg Spectralis in clinical use. After demonstrating on several patients, the scientist asked me if I thought it were possible for someone to take an OCT image of themselves. I pivoted the monitor, control panel, and footswitch around so I could operate the OCT from the patient chair and then captured some images of my own retina. I was showing off a little and smugly cautioned the NASA doctor that this was a difficult feat that only an experienced ophthalmic imager could perform. After all, I’ve been doing this for over thirty years. She paused for a moment and then said, “With all due respect, astronauts are some of the smartest and most talented people on earth. They shouldn’t have any difficulty performing OCTs on themselves after a some brief training.” Suddenly I didn’t feel so smug.
A year or so later, the Spectralis arrived at the International Space Station and it looks like she was right. I heard from some colleagues at Heidelberg that the astronauts were given less than 30 minutes of training on the instrument and mastered it quickly!
It’s pretty cool knowing that astronauts are performing ophthalmic imaging on the International Space Station. I wonder if they ever see any resemblance between the eye and celestial bodies?
Disclosure: I have no financial or proprietary interest in the Heidelberg Spectralis.
Here are some links on the condition that’s effecting the vision of astronauts and the use of diagnostic imaging on the space station:
When performing fundus photography or angiography, patients often ask about the technology used to help diagnose their ocular condition. After explaining that it’s a form of photography, the conversation will often turn to cameras. Patients sometimes ask for advice on what type of camera to buy for personal use. Often they’ll tell me about a particular camera they have and will invariably say “the camera takes great pictures”.
I’ve always found this expression and the concept behind it quite amusing. It assumes the person looking through the viewfinder and pressing the shutter button has nothing to do with it! On several occasions these conversations took place at a VA hospital while photographing vets. They’ll talk about having purchased a camera overseas, such as a Voigtlander, Zeiss Contax, or Leica in Europe during WWII, or a Nikon while stationed in Japan, Korea, or Vietnam. Without fail, they’ll tell me that “the camera takes great pictures”. All are quality cameras with good optics, but none of them are capable of taking pictures on their own. Someone has to compose the image and press the shutter.
A related misconception has occurred in ophthalmic imaging over the past decade. With all the automated features such as eye tracking, sampling, auto-alignment and auto-exposure, etc. in the current crop of instruments, there is a perception that retinal imaging is simple and easy to perform. The implication is that the machine takes the picture, not the operator.
It’s true that recent advancements in technology have improved and simplified image capture, but I still believe that skilled photographers produce the best diagnostic images. I once had a conversation with an overly-enthusiastic OCT salesman who claimed his instrument was better than the competition. As proof, he showed me two images of the same patient taken with two different OCT instruments. “See”, he said, “The competition’s instrument missed the pathology”. I corrected him saying that it wasn’t the instrument that missed the pathology, but the operator.
High resolution line scan of a small retinal arterial macroaneurysm captured using the free scanning technique.
This sparked an interesting debate. I argued that a skilled OCT operator, given appropriate direction from the ordering physician, would not have missed the area of interest. Ultimately we agreed it’s up to the operator to make the best use of the technology they have available.
Several famous photographers have weighed in on the relationship between camera and photographer in producing great images. I love these quotes:
“You don’t take a photograph, you make it.” Ansel Adams
“The camera doesn’t make a bit of difference. All of them can record what you are seeing. But, you have to SEE”. Ernst Haas
“The camera is an instrument that teaches people how to see without a camera.” Dorothea Lange
“Photography is the art of observation… I have found it has little to do with the things you see and everything to do with the way you see them.” Elliot Erwitt
“There is nothing worse than a brilliant image of a fuzzy concept.” Ansel Adams
And finally, whenever someone states, “This camera takes great pictures”, I reply with another common quote that’s been attributed to several people, including boxing trainer Roger Mayweather, basketball great Charles Barkley, and possibly even Confucius:
“It ain’t the tools, it’s the carpenter”.
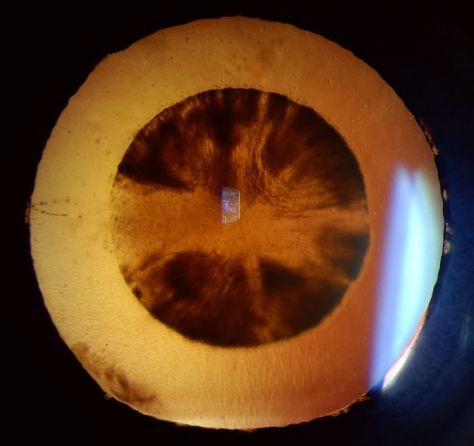
Slit-lamp photograph of dislocated intraocular lens implant and iris erosion shown in transillumination. Slit-lamp imaging relies on advanced photographic lighting techniques to accurately document the condition of the eye.
Voigtlander camera image from Wikimedia Commons: https://en.wikipedia.org/wiki/File:Vitorets.JPG#filelinks
Did you ever wonder how ophthalmic diagnostic findings get their names? If you feel like there is no rhyme or reason to the naming conventions used in ophthalmology, you are not alone. Ophthalmology (and medicine in general) does not have structured system of nomenclature like some other sciences.
For example, the field of chemistry utilizes the periodic table of elements to organize and classify fundamental information. Biology employs Linnaean Taxonomy, which is an organized hierarchical system of classification including kingdom, phylum, class, order, family, and genus, to differentiate and name species. It was established and organized by Carl Linnaeus in the mid 1700’s and results in a naming convention known as binomial nomenclature.
In binomial nomenclature, this common Tiger Swallowtail butterfly is known as Papilio Glaucus. It was classified and named by Linnaeus himself in 1758. Papilio is latin for butterfly and glaucus means blue.
Human anatomy and medicine is a different story however. Historically there has been controversy, disagreement, language differences, and confusion amongst anatomists regarding universal terminology. To address this, there have been attempts to standardize terminology in human anatomy. Nomina Anatomica was the international standard on human anatomic terminology from 1956 until it was replaced by Terminologia Anatomica in 1998. But in ophthalmology, as in much of medicine, there is no universal system of classification for ocular anatomy, clinical findings, or diseases. It’s a bit of a “free-for-all”. In the late nineteenth century some 50,000 terms for various body parts were in use. The same structures were described by different names, depending on the anatomist’s background: school, language, culture, traditions, etc.
Let’s take a look at some of the ways that diseases are named in ophthalmology. Clinical findings may be named for their anatomic location, clinical appearance, etiology, disease process, or end result. They may also be based on etymologic roots or finally, eponyms.
A common and logical diagnostic naming convention is simply descriptive of a disease process like vitreomacular traction or corneal erosion.
Or it could be the anatomic result of those processes such as a macular hole that results from vitreomacular traction or a corneal ulcer that arises from erosion.
Some terms are based on clinical appearance, either the literal appearance or a resemblance to something else. Pink eye or floppy lid syndrome are conditions that are literally descriptive of their appearance.
Conditions like bear tracks, bullseye maculopathy, cotton wool spots, morning glory nerve, birdshot choroidopathy, and several others often bear a resemblance to something that would be commonly recognized or understood.
Other names may be based on etymology, which means they originate from traditional Greek or Latin root words.Heterochromiais a good example as it comes from the Greek roots heteros which means different, and chroma which means color.
Cataractis an interesting term that may be related to the opaque lens’ resemblance to rushing water of a waterfall, or possibly to one of the earlier etymologic roots meaning a covering or impediment.
Some conditions are probably better known by the acronym representing the full name: ARN, CHRPE, APMPPE, etc.
Finally, many conditions are based on eponyms meaning they are named for a person, usually the person that first identified or described the condition in the literature. Eponyms are a longstanding tradition in science and medicine, and being awarded an eponym is considered an honor.
Anatomists seem to have been especially fond of naming structures for themselves as seen by the many eponymous anatomic terms in ophthalmology: Bowman’s Membrane, Descemet’s Membrane, Canal of Schlemm, Annulus of Zinn, Schwalbe’s Line, Tenon’s capsule, and Bruch’s Membrane to name just a few.
Purtscher’s retinopathy is an example of a well-known eponym in ophthalmology. In 1910, Austrian ophthalmologist, Otmar Purtscher (1852-1927) described a retinopathy of bilateral peripapillary patches of retinal whitening and hemorrhages after compression injury to the head.
Eponyms extend beyond anatomy into diagnoses as well. Conditions have been named for Sjögren, Krukenberg, Stargardt, Marfan, Elschnig, Thygeson, Vogt, Cogan and countless others. We certainly shouldn’t overlook Austrian ophthalmologist Ernst Fuchs, who described several conditions and has his eponym associated with many of them. Eponyms may also be proper names of places ( Lyme Disease, North Carolina Macular Dystrophy) or famous patients: Lou Gehrig’s Disease (amyotrophic lateral sclerosis) or Tommy John surgery (named for Major League pitcher, first person to undergo the procedure).
With all these names and egos involved, there has often been confusion and controversy over who was the first to fully describe a condition. Bergmeister’s papilla and Mittendorf dot are eponyms given to remnants of opposite ends of the embryonic hyaloid artery. Vogt-Koyangi-Harada disease is named for three investigators who independently described different manifestations of the same underlying condition. Stevens-Johnson syndrome, named for pediatricians Albert Mason Stevens and Frank Chambliss Johnson, also has several other eponyms associated with it including names such as: Baader, Fiessinger, Rendu, Fuchs, Klauder, Neumann and Hebra – whew! Further confusing things are hyphenated or double surnames such as Robert Foster-Kennedy (Foster-Kennedy syndrome ) and Roger Wyburn-Mason (Wyburn-Mason syndrome).
Dilated and tortuous retinal vascular abnormalities are a hallmark of Wyburn-Mason syndrome. Findings also include arteriovenous malformations in the midbrain in this rare condition named for British physician Roger Wyburn-Mason who described it in 1943. It is also known as Bonnet-Dechaume-Blanc syndrome, named for the group that described it in 1937.
In fact, Wyburn-Mason syndrome had been previously described in the French literature and is also known as Bonnet-Dechaume-Blanc syndrome. So the correct eponym may depend on what language you speak.
Eponyms are often controversial, especially when questions arise about the moral and ethical character of eponymous honorees. There has been sparring in the literature for years over the use of eponyms and the worthiness of some of the individuals that have conditions named for them. Pulido and Matteson ask the question, “Is it worth having eponyms at all?” in an editorial in Retina in 2010. They go on to state, “Although they can function as a memory aid, they do not enhance understanding of disease…. It is best henceforth to not name new diseases with eponyms and to start moving away from their use completely.”
Stargardt disease was described by Karl Bruno Stargardt in 1909. In 1997, researchers identified a mutation in the ABCA4 gene as the cause for this hereditary retinal disorder. Many hereditary diseases are now being referred to by their identified gene mutation rather than an eponym.
Wikipedia lists some of the pros and cons of eponyms in eponomously named diseases and briefly talks about current trends:
“The current trend is away from the use of eponymous disease names, towards a medical name that describes either the cause or primary signs.”
“The scientific and medical communities regard it as bad form to attempt to eponymise oneself.”
Then there is Stigler’s Law of Eponymy, which states, “No scientific discovery is named for the original discoverer.” As proof, Stigler freely admits that others postulated the idea before he named it for himself! In describing Stigler’s Law, Malcolm Gladwell stated, “We think we’re pinning medals on heroes. In fact, we’re pinning tails on donkeys.”
David Cogan talked about the pitfalls and limited life of eponymous designations in an editorial in the Archives of Ophthalmology in 1978. Yet Cogan-Reese syndrome was named for him and Algernon Reese many years ago.
When a new designation, ICE syndrome, was suggested as a unifying term to replace Cogan-Reese syndrome, Chandler syndrome, and essential iris atrophy, Cogan was quoted by William Spencer in another editorial in Archives: “Better a descriptive name, if that is possible, and an eponym if it is not possible. Now the syndrome described by Al Reese and me is characterized by nodules, unilateral glaucoma, Descemet’s membrane and endothelial extension; why not call it by the acronym NUDE syndrome? This would give it sex appeal and put the Archives right up there with Esquire.” Cogan’s response suggests he thought eponyms still have their place – especially when it came to one named for himself!
Surprisingly, these trends and opinions haven’t prevented the coining of new eponyms in ophthalmology. In 2013, a new anatomic layer of the human cornea was first described by Harminder Dua in the journal Ophthalmology. There was even a big splash in the mainstream scientific news and social media about this exciting new discovery and the investigator who identified it. As you may have already guessed, the finding is called Dua’s layer. He named it for himself!
Despite all the controversies, confusion, and egos involved, it seems as if eponyms in ophthalmology are here to stay, at least for now. So try not to be confused or frustrated when comparing Fuchs’ corneal dystrophy with Fuchs’ heterochromic iridocyclitis, or if you have difficulty remembering whether it is Best’s or Behcet’s disease that has macular vitelliform lesions. We might as well embrace these long-established eponyms – warts and all.
Resources Here are some great resources to look up information on eponyms in medicine and ophthalmology:
Whitmore I. Terminologia anatomica: new terminology for the new anatomist. Anat Rec. 1999 Apr 15;257(2):50-3.
Lamy R, Dantas AM. [Anatomical nomenclature in ophthalmology]. Arq Bras Oftalmol. 2008 May-Jun;71(3):446-58. Portuguese.
Pulido JS, Matteson EL. Eponyms: what’s in a name? Retina. 2010 Nov-Dec;30(10):1559-60.
Grzybowski A, Rohrbach JM. “Eponyms: what’s in a name”. Retina. 2011 Jul-Aug;31(7):1439-42; author reply 1442-3.
Grzybowski A, Rohrbach JM. [Should we abandon the eponym ‘Wegener’s granulomatosis’? A historical excursion]. Klin Monbl Augenheilkd. 2011 Jul;228(7):641-3.
Cogan DG. The rise and fall of eponyms. Arch Ophthalmol. 1978 Dec;96(12):2202-3.
Eagle RC Jr, Font RL, Yanoff M, Fine BS. Proliferative endotheliopathy with iris abnormalities. The iridocorneal endothelial syndrome. Arch Ophthalmol. 1979 Nov;97(11):2104-11.
Spencer WH. Proliferating terminology and the NUDE syndrome. Arch Ophthalmol. 1979 Nov;97(11):2103.
Ophthalmic photography has long played an important role in the documentation and diagnosis of ocular diseases. Ocular photography is used to record medical conditions, track disease progression, and create illustrations for publication and education. The primary role of ophthalmic imaging however goes well beyond documentation in its ability to aid in diagnosis of a broad range of eye conditions. Treatment plans derived from the diagnostic information provided by ophthalmic images have benefited countless patients, as ophthalmologists use images for decision making purposes on a daily basis, and in some cases, rely on photographs as a “road map” to guide therapy.
The history of ocular photography dates back to the late 1800’s when Jackman and Webster described a technique for photographing the retina of a living human subject. The next fifty years witnessed a slow advancement in instrumentation and techniques. Photographic results were mostly inadequate due to slow film speeds, long exposures, and inconsistent light sources. In the 1950s electronic flash and 35mm cameras were adapted to ophthalmic instruments and modern ophthalmic photography was born.
There is a compelling connection between this photographic discipline and our subject, the human eye; a connection that goes beyond the obvious parallels between eye and camera, cornea and lens, iris and aperture, retina and film. We use the visual art of photography to identify problems in another visual system – the eye itself. Optical instruments used to examine or photograph the eye often utilize the optics of the subject eye to help in visualizing the target pathology.
Ophthalmic photography can at times be simple or incredibly complex. Ocular tissues can be opaque, translucent, or transparent and may require different strategies to record these structures photographically. Enhancement of anatomic features is sometimes necessary, and can be achieved by using fluorescent dyes, monochromatic light, or specialized optical devices and techniques to adequately document subtle pathology that would otherwise not be visible.
Creativity and aesthetics have their place in this field and many ophthalmic images transcend their scientific purpose and achieve artistic merit, but it can be heartbreaking when the most photogenic or aesthetically pleasing subjects present themselves because a patient’s vision is severely compromised. Enthusiasm for creative imaging can suffer in the context of tragic loss of vision. This is balanced however, against those times when an imager captures great images that help preserve a patient’s vision. Unfortunately not all images will be of sufficient quality to warrant public display or publication. The challenge for ophthalmic photographers is to provide consistent clinical images of adequate diagnostic quality, even under adverse conditions.
By providing support for education, research, and clinical eye care activities, ophthalmic photographers have been an integral part of the professional eye care community for decades. As new diagnostic imaging and treatment modalities are developed, the role of the ophthalmic imager will evolve and continue to play an important role in the preservation of sight.
I first heard this expression many years ago when a retina specialist was explaining the results of a fluorescein angiogram to a patient and her family. He went on to explain that her retina represented the “film” in the camera and that it was swollen with fluid and wrinkled, which was the cause of her blurred vision. Everyone present easily understood the analogy, as 35mm cameras were commonplace at the time. The idea of warped or wrinkled film resonated as an analogy.
Although it was my first time hearing this comparison, it was not a new or unique concept. The compelling connection between the eye and camera dates as far back as the 16th century when Leonardo DaVinci drew a comparison between the camera obscura and the human eye. In the next century, Della Porta, Cigoli, and Descartes also made a similar connection in their writings on optics and vision.
With the introduction of practical photographic methods in 1839, the analogy soon extended beyond the optical comparison between eye and camera obscura to include the comparison between vision and imaging. As photography and cameras quickly grew in popularity, scientists, physicians and ophthalmologists such as Helmholtz and LeConte advanced the analogy between photographic camera and the eye.
“The further explanation of the wonderful mechanism of the eye is best brought out by a comparison with some optical instrument. We select for this purpose the photographic camera. The eye and the camera: the one a masterpiece of Nature’s, the other of man’s work.”
Joseph LeConte
From the earliest days of photography, several investigators sought to use the camera to document the condition of the eye. Due to the technical limitations of available photosensitive materials and the difficulty in illuminating the interior of the eye, fundus photography became the “holy grail” of medical imaging. Over the next several decades there were incremental advances in optical instrumentation and photographic processes, all moving steadily towards practical examination and photography of the eye. The most notable of these milestones was the 1851 introduction of the ophthalmoscope by Helmholtz.
Lucien Howe, one of the early pioneers in fundus photography echoed the idea of eye as camera in his 1887 article in which he described having captured the first recognizable fundus photograph:
“We know that the eye itself is a camera, and when placed behind an ophthalmoscope it has pictured upon the retina an image of an eye observed.”
Lucien Howe
The analogy was taken yet a step further by Mann who presented a paper utilizing animal eyes as an actual camera by placing photographic film against an aperture cut in the posterior pole of the globe.
“The main object has been to demonstrate that the eye can actually be used as a camera, a fact which is of interest chiefly because of the frequent comparison between the two.”
William Mann
From that point on there were several milestones in the evolution of both photography and ophthalmic photography that culminated in reflex-free fundus cameras equipped with electronic flash by the 1950’s. The modern fundus camera revolutionized ophthalmic photography and provided the platform for the important development of fluorescein angiography techniques by Novotny and Alvis in 1959. Optical coherence tomography has further revolutionized ophthalmic imaging, but fundus photography and angiography remain vital tools in the diagnosis and treatment of ocular disease.
In today’s wireless and digital age, the analogy of eye as camera may not be as universally accepted as it was a generation ago. Most 35mm cameras had a spring-loaded pressure plate on the film door to ensure the film was held flat and firmly in place. It was easy to envision the concept of a piece of film (or a retina) being wrinkled, torn, or warped.
Today’s digital cameras do not open to reveal the fixed sensor inside so the analogy doesn’t resonate as well. Yet the optical comparison between the eye and camera lens still rings true today, even with sophisticated scanning instruments such as SLO and OCT.
“The eye is like a camera.”…. Since the days of DaVinci, this idea has been echoed countless times by philosophers, artists, ophthalmologists and photographers. As an ophthalmic photographer, I consider myself fortunate to have spent a career photographing the human eye: one camera being used to preserve the capabilities of the other.
“The camera exists because men were intrigued by the function of the eye and wished to be able to reproduce on a permanent record that which the eye enabled the brain to record. How appropriate then that ophthalmology has turned the camera into a valuable tool for recording the structures of the eye.”
R. Hurtes
“The eye is like a camera.”
References
Wade NJ, Finger S. The eye as optical instrument: from camera obscura to Helmholtz’s perspective. Perception 2001; 30:1157-1177
LeConte J. The Eye as an Optical Instrument. from Sight: An Exposition of the Principles of Monocular and Binocular Vision. 1897
Howe L. Photography of the interior of the eye. Trans Amer Ophth Soc. 23:568-71 July 1887
Mann WA. Direct utilization of the eye as a camera. Trans Am Ophthalmol Soc 42:495-508, 1944
Novotny HR, Alvis DL. A method of photographing fluorescence in circulating blood of the human retina. Circulation. 24:82, 1961
Meyer-Schwickerath, G. Ophthalmology and photography. AJO 66:1011, 1968
Bennett TJ. Ophthalmic imaging – an overview and current state of the art. Journal of Biocommunication, 32(2):16-26, 2007.
Bennett TJ. Ophthalmic imaging – an overview and current state of the art, part II. Journal of Biocommunication, 33(1):3-10, 2007.
Hurtes R. Evolution of Ophthalmic Photography. International Ophthalmology Clinics. 1976; 16(2):1-22
Although it may seem like a recent phenomenon, the photographic self-portrait has been with us since the dawn of photography. Perhaps the earliest known “selfie” was taken by Hippolyte Bayard (Portrait of a Drowned Man), a Frenchman who claimed to have invented a photographic process prior to the Daguerrotype. The same can be said of William Henry Fox-Talbot (The Reading Establishment).
In recent years, the photographic self-portrait has exploded in popularity into a global phenomenon, fueled by social media sites such as Facebook, Instagram, Twitter, Snapchat, and others. It is estimated that over one million “selfies” are taken every day. A recent search of Instagram returned over 211 million photos with the hashtag “#selfie”. The term “selfie” is believed to have originated in Australia and has been elevated from internet slang to our common vernacular and even inclusion in several formal English dictionaries. In fact, selfie was Oxford Dictionary’s word of the year for 2013!
Everybody seems to be getting into the act including celebrities, politicians, and even the Pope! Selfies are even popular in space. Astronauts have shared several spacewalk selfies online, and last year, NASA promoted a global selfie project to celebrate Earth Day. They solicited over 36,000 selfies from around the world and created an interactive composite image that can be viewed on their website.
The selfie is so ubiquitous in today’s pop culture that cell phones and digital cameras often include built-in selfie-friendly apps and features such as extra wide angle lenses, articulating screens or front facing screens that facilitate the selfie pose. You can also purchase selfie sticks to extend the camera to a better vantage point. These popular items go well beyond the simple self-timer found on many cameras of yesteryear. Selfies are often purposely self-deprecating, campy, cheesy, or irreverent. They are meant to be spontaneous and fun and are not usually taken very seriously. The selfie craze has even spawned the infamous “duck face” pose.
Despite the fun and seemingly harmless spirit behind them, there is a belief that taking selfies can be a sign of narcissism rather than simple self-expression. There is also some concern it can be addicting and unhealthy. But there is a growing trend in telemedicine where patients can take and forward selfies to their doctors to help diagnose or triage the urgency of their condition. So maybe there are some legitimate uses for selfies.
As a life-long photographer, I’ve taken my share of selfies over the years. I’ve even attempted a few with the equipment I use for diagnostic ophthalmic photography. Some are goofy, and in the spirit of social media selfies. Some are more practical.
Most ophthalmic imaging devices are not what you’d normally consider selfie friendly, at least not in terms of taking a photo of one’s own eyes. Because the optics of these devices are designed for photographing curved surfaces found in the interior of the eye, they usually create distortion when backed up an appropriate distance to take a facial portrait. The effect of this distortion eliminates the need for a goofy facial expression if your goal is just to post a unique selfie on the internet!
But what about useful diagnostic or artistic photos of your own eyes, photos that go beyond distorted face selfies? It’s not only possible, but surprisingly good images can be obtained with some devices. Non-mydriatic instruments with a monitor that can be pivoted toward the patient/photographer lend themselves to self-imaging, while those with an optical viewfinder (fundus camera) or fixed monitor position (Cirrus) do not. I’ve been able to obtain eye selfies with the Zeiss Stratus, Heidelberg HRT, Heidelberg HRA/OCT, Clarity RetCam, Tomey specular microscope and various handheld external cameras. But, you might ask, “So what?” or “Why?”
Well, there have been times when I needed to check a device during maintenance or a software upgrade and it was convenient to use myself as the patient. Sometimes while training staff to use a device, I’ll demonstrate the procedure on myself. Other times, I’ve needed a quick example of a “normal” eye for a lecture like those above.
Surprisingly, the ability to take eye “selfies” has helped me identify and track pathology in my own eyes. Two years ago I suffered an idiopathic retinal tear with avulsed bridging vessel and persistent vitreous hemorrhage. This was successfully treated with vitrectomy. Like many patients, I developed a cataract after the vitrectomy. I also began to notice some distortion that corresponded to progression of an epiretinal membrane (ERM) in the same eye.
Any time I noticed a change in vision I would repeat an OCT on myself. Over the course of six months I tracked an increase in thickness of about 100 microns. The cataract also progressed and I was scheduled for cataract surgery. Two weeks prior to surgery I noticed a very subtle change in vision and sat down at the OCT like I’d done several times in the past. The OCT detected some cystoid macular edema (CME) from the ERM. Picking up the CME prior to cataract surgery was very beneficial. Preexisting CME can be exacerbated by cataract surgery, so my surgeon began a course of treatment that reduced the edema. My OCT selfies likely helped us avoid more severe or persistent edema by catching it in advance.
Cataract surgery went as planned, but within a few hours of my procedure I began to notice a new visual abnormality: a paracentral gray scotoma. Upon arriving at the clinic the next day for my post-operative check, I immediately did an SLO/OCT selfie and identified an unusual finding that corresponded directly to the scotoma.
SD-OCT demonstrated an area of hyper-reflectivity in the middle retinal layers just temporal to the fovea (green arrows) and the IR reflectance image showed a distinct dark gray lesion. Fortunately, the scotoma began to fade within a few days and so did the lesion. The jury is still out on the exact cause of the lesion but the selfies have enabled us to track improvement of my condition and possibly publish a case report. We believe it may be a case of paracentral acute middle maculopathy (PAMM), a recently described variant of acute macular neuroretinopathy (AMN). It’s rare enough, that I was able to present it at the OPS Rare Case Symposium in Ann Arbor.
As you can see, image quality can be quite good with a little practice. So good in fact that I’ve received a bill from my institution for OCT images that I’ve performed on myself! Here is a double selfie video of a Spectralis IR fundus image showing how easy it is to capture my own epiretinal membrane.
“
I’m beginning to think maybe I should stop taking selfies of my own eyes. After all I keep finding abnormalities! But there is a growing trend in telemedicine where patients can take and forward selfies to their doctors to help diagnose or triage the urgency of their condition.
Ophthalmic Photographers taking diagnostic selfies: obsessive, silly, or beneficial?



























 When a new designation, ICE syndrome, was suggested as a unifying term to replace Cogan-Reese syndrome, Chandler syndrome, and essential iris atrophy, Cogan was quoted by William Spencer in another editorial in Archives: “Better a descriptive name, if that is possible, and an eponym if it is not possible. Now the syndrome described by Al Reese and me is characterized by nodules, unilateral glaucoma, Descemet’s membrane and endothelial extension; why not call it by the acronym NUDE syndrome? This would give it sex appeal and put the Archives right up there with Esquire.” Cogan’s response suggests he thought eponyms still have their place – especially when it came to one named for himself!
When a new designation, ICE syndrome, was suggested as a unifying term to replace Cogan-Reese syndrome, Chandler syndrome, and essential iris atrophy, Cogan was quoted by William Spencer in another editorial in Archives: “Better a descriptive name, if that is possible, and an eponym if it is not possible. Now the syndrome described by Al Reese and me is characterized by nodules, unilateral glaucoma, Descemet’s membrane and endothelial extension; why not call it by the acronym NUDE syndrome? This would give it sex appeal and put the Archives right up there with Esquire.” Cogan’s response suggests he thought eponyms still have their place – especially when it came to one named for himself!




















